The following article was originally written for plastic surgeons, describing our technique for asian double eyelid surgery. Since its original publication in 1999, it has remained one of the highest ranked medical articles written for the eyelid surgeon on Google under search terms “asian eyelid surgery” and “asian blepharoplasty” as of September 2009. http://emedicine.medscape.com/article/1282140-overview.
We have translated it for the lay person. Photos will follow. We will expand on the article as permitted by space.
We strongly prefer the word “eyelid surgeon” for the overlapping medical specialties with interest in eyelid surgery. Besides plastic surgeons, other specialities engaged in eyelid surgery include opthalmologists (“eye plastic surgeons”), otolarynologists or ENT (“facial plastic surgeons”), dermatologists and oral surgeons (“cosmetic surgeons”).
To avoid confusion, we limit the use of the word “plastic surgeon” to a surgeon whose training is sanctioned by the American Board of Plastic Surgery.
The original article translated below was peer-reviewed (reviewed by plastic surgery expert colleagues) for accuracy. Acknowledged authorities in the field of plastic surgery corrected inaccuracies prior to approval for publication.
EDIT: Due to search engine guidelines, a direct translation is not permitted. A general translation is posted.
Asian Eyelid Plastic Surgery (Asian blepharoplasty)

Before and after: Asian eyelid surgery, asian nose surgery, chin implant, buccal (cheek) fat removal). Detailed description to below.
Twenty two year old patient for anchor eyelid crease surgery, asian rhinoplasty, chin implant and buccal fat removal.






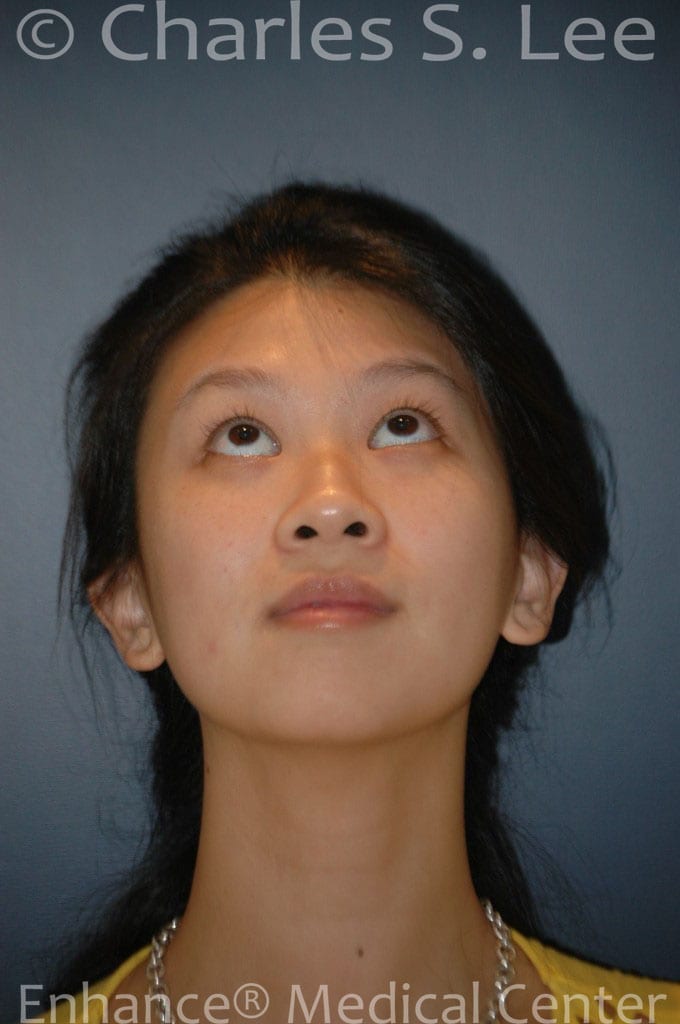

Anchor blepharoplasty: Prior suture method crease procedure was revised. Sutures removed with no difficulty, all sutures were removed and minimal scarring was noted within the operative field. Larger folds were set in accordance to the size of the patient’s eyelid cartilage (tarsal plate), which is 7mm unstretched skin, or 9mm with the skin on stretch. The right brow was slightly lower so additional eyelid skin was removed to accommodate the smaller right crease. The skin below the crease incision was smoothened out and “anchored” to make the skin smooth, and to minimize the risk of crease failure (“anchor blepharoplasty” is a unique variation of the asian eyelid surgery, or asian blepharoplasty).
The rhinoplasty (discussed under the blog section of asian nose surgery – asianplasticsurgeryblog.com), is performed in the “closed” technique, with no external scar between the nostrils. The bridge is raised using a silicone plastic implant (2{0fd4121d5216b280473771676d11ae34909381d9377f36f96353e02149c70f16} extrusion rate, in our series). The tip graft to raise, strengthen, and better define the tip is accomplished using a large cartilage graft, placed through the right nostril. We currently avoid the “open” incision due to the stress placed on the central skin, which can lead to significant scarring. The nostrils are narrowed using the incision placed in the nostril groove.
The chin implant is silastic, and placed through an incision within the gumline of the mouth. The chin is slightly undercorrected to avoid discomfort and lower lip distortion.
Buccal, or cheek fat, is removed through an incision on the inside of the mouth. More was removed from the right side, due to asymmetry, common in 80{0fd4121d5216b280473771676d11ae34909381d9377f36f96353e02149c70f16} of the population.
Introduction
Asian double eyelid surgery refers to placement of a crease in the upper lid of Asian patients who lack such a crease. Patients request the procedure in order to apply makeup with more ease, look more alert, or look more bright-eyed. In modern American society, Westernization of the upper lid is not the goal of the procedure.
History
The earliest reference to the procedure occurred in Japan in the 1890’s. A patient born with a crease in one eyelid had a crease placed in the other eyelid using a suture technique. In Japan, the evolution of this procedure was published extensively until WWII.
In the English language, the first references were from Sayoc, and the first American to publish this was D. Millard in 1955 (the author’s plastic surgery chairman at the University of Miami). Leabert Fernandez, a plastic surgeon in Hawaii, described the modern double eyelid operation, in which an full incision was made and the skin attached to the levator (eyelid opening muscle). This is perhaps the most popular technique used even today, and Fernandez can be considered the developer of the modern asian eyelid operation.
Robert Flowers, also in Hawaii, developed an extensive refinement of Fernandez procedure. The procedure, which Flowers refers to as the “Anchor” method, focuses on creating a smooth, unwrinkled skin in the sub-crease, platform area (skin between the eyelashes and the crease). This is the authors’ preferred technique.
Anatomy
The primary difference between the Occidental crease and the Asian crease has been pointed out in great detail anatomically.
A simplified understanding of the crease is as follows. The upper eyelid opens itself by an elevating muscle, called the “levator”. The eyelid crease is formed at the attachment point of this muscle to the eyelid. If it attaches very low (close to the eyelashes), the crease will be very close to the eyelashes, i.e., very small. If the attachment point is higher, then the crease will be higher. In Asians, the insertion point, if high enough to be visible, generally attaches 5-10mm from the lashes. In Occidentals, this distance is 10mm or higher.
The surgical strategy for creating an eyelid crease in the Asian eyelid is to attach the skin, at the desired crease height, to this lifting (levator) muscle.
Two broad categories of surgery to accomplish this technique are the “full incision method” and the “suture method”. There are several variations within these two techniques, and the author discusses his preferred technique within each broad category.
Treatment
The two broad categories include the open, or full incision technique, and the suture technique.
The author prefers the suture method in cases where the skin and underlying muscle are thin and there is no excess overhanging skin or droopiness of the eyebrow. Typically the candidate is a patient in his/her mid’20’s or younger and want a medium to small size fold. Older patients can be candidates in select cases, especially if a large fold is not the goal. Many male patients are candidates for this technique due to the minimal visible scarring and their tolerance for smaller size folds.
In addition, this technique is particularly applicable to patients who have intermittent or slightly indistinct folds.
Patients who are not candidates for the suture techniques include patients with pre-existing eye muscle conditions (ptosis, retraction), or excess upper eyelid skin.
In our experience, the suture method, and in particular the Double -sutures and twisting technique- (DST) does not lead to extensive internal scarring or difficulties with subsequent surgeries. However, surgeons not familiar with the technique or the anatomy of this complex area should by all means avoid this procedure.
The incision method is the default procedure of choice for patients who are otherwise not candidates for the suture techniques. The advantages of the incision technique include precision in the size and shape of the crease, flexibility in removal of excess skin and fat and permanence of the procedure. The drawbacks to the technique include potential visible scarring, irreversibility, longer recovery time, and dependence on the artistic ability of the surgeon.
The learning curve for the technical as well as the artistic aspect of the incisional double eyelid operation is quite lengthy. In addition to experience, we would add instruction on proper technique as well as innate artistic talent as equally important in obtaining a good outcome. As a famous plastic surgeon, Ralph Millard (http://en.wikipedia.org/wiki/Ralph_Millard said, “it’s not how many you do, but how you do it.”






{kind=link}
{kind=link}
{kind=link}